Laparoscopic colectomy
Jan 14, 2025Since 1992, laparoscopic colorectal surgery in our country has made great progress. It has rapidly expanded from a procedure that was originally only carried out in depth in some large teaching hospitals to grassroots hospitals and has achieved remarkable results.
Currently, laparoscopic colectomy has become one of the common methods for treating colon diseases and is widely used in clinical practice. Although laparoscopic surgery has many advantages, it still faces some challenges, such as high surgical difficulty and strict technical requirements for surgeons.
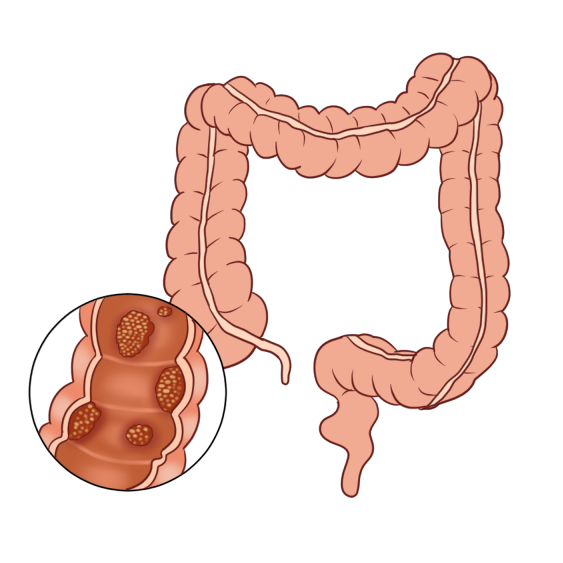
Many patients with intestinal diseases such as colon cancer and intestinal obstruction need to undergo "laparoscopic colectomy". Let's take the left hemicolectomy as an example to briefly understand laparoscopic colectomy.
1. First, assess the condition and design the resection range.
2. Establish pneumoperitoneum
The doctor then makes a small hole about 1 cm long next to the belly button and inserts the camera to see if it has penetrated into the abdominal cavity. If it has, the doctor will start to connect the inflation device and inject carbon dioxide into it, with the purpose of making the belly bulge for further surgery.
3. Exploring the abdominal cavity
After establishing pneumoperitoneum, the doctor can see the abdominal organs and tissues on the display screen through the camera. Then, several small holes (about 0.5-1cm long) are gradually created on the skin around the diseased intestines as auxiliary operation holes. Doctors can insert various instruments, such as forceps and suction devices, through these small holes. Then, the doctor explores the general situation of each organ in the abdominal cavity under the camera, observes whether there are any abnormalities, and finds the specific location of the diseased intestines. If it is a tumor lesion, it is also necessary to consider whether there is distant metastasis.
4. Isolation and resection of diseased intestinal segment
After finding the diseased intestinal segment under laparoscope, the intestine is separated first to form a free state, and then the scope of intestinal resection is considered according to the nature of the lesion. If the patient is a tumor, it is necessary to remove a part of the normal intestine in addition to the diseased intestinal segment. The specific operation steps are shown in the following steps:
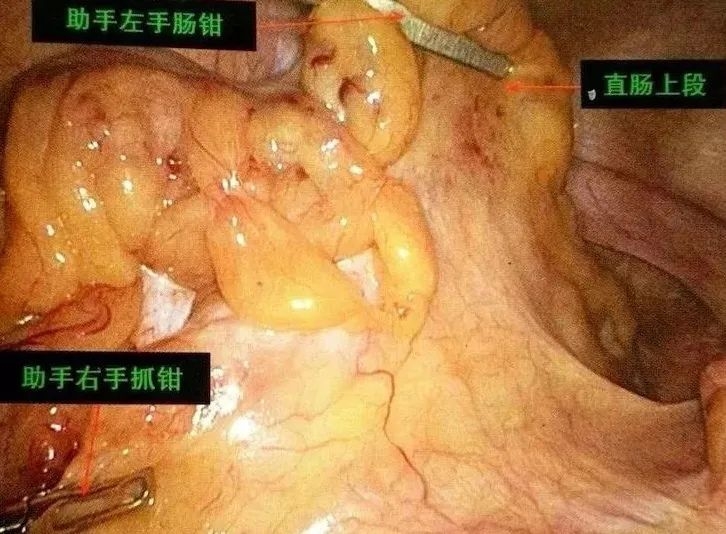
Retract and stretch the sigmoid colon mesocolon
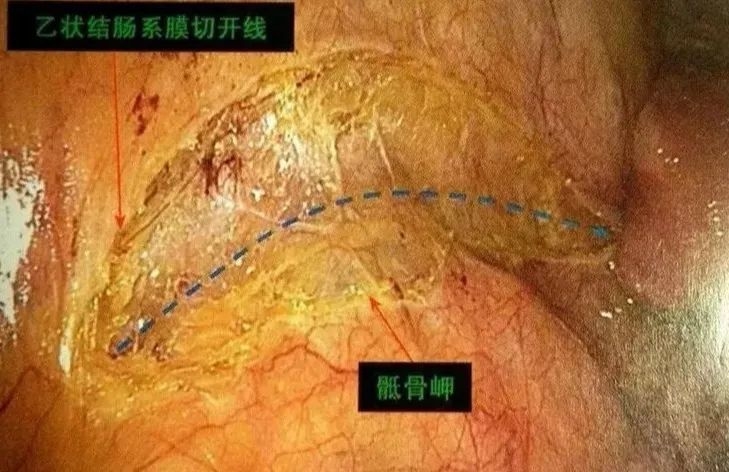
Design cutting line

Open the inner yellow-white junction and enter the left colonic space
To the left, head side to fully expand the gap
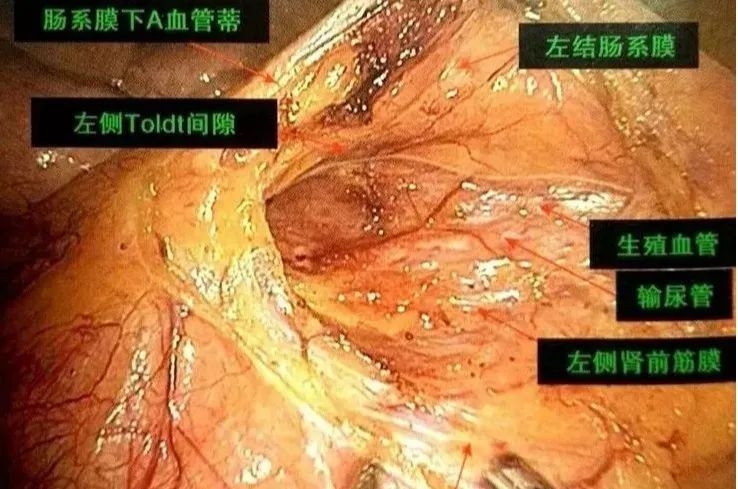
Reach the root of IMA, clear lymph and cut blood vessels

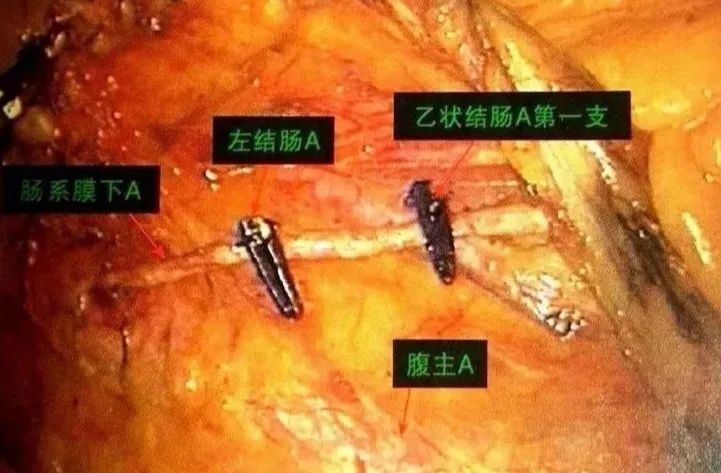
Depending on the situation, open the vascular sheath and highly selectively cut off the blood vessels

Preserve the main branch of IMA and highly selectively divide the left colic and sigmoid arteries
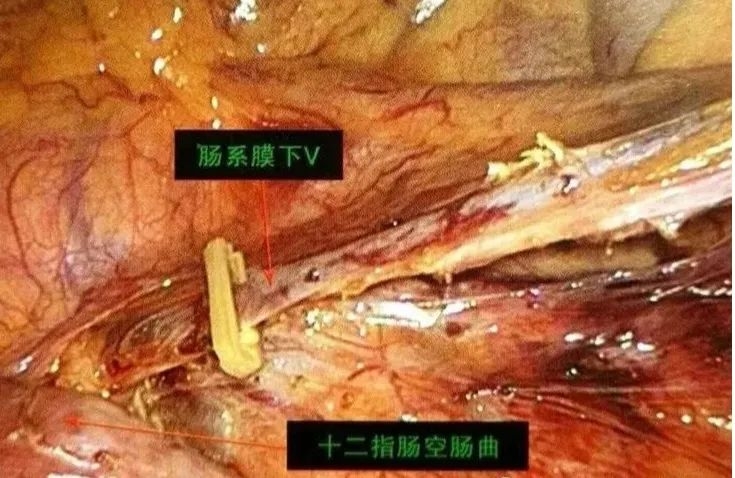
Inferior mesenteric vein
Lift and flatten the transverse colon mesentery

Open the transverse colon mesentery at the lower edge of the pancreas and enter the lesser omental sac
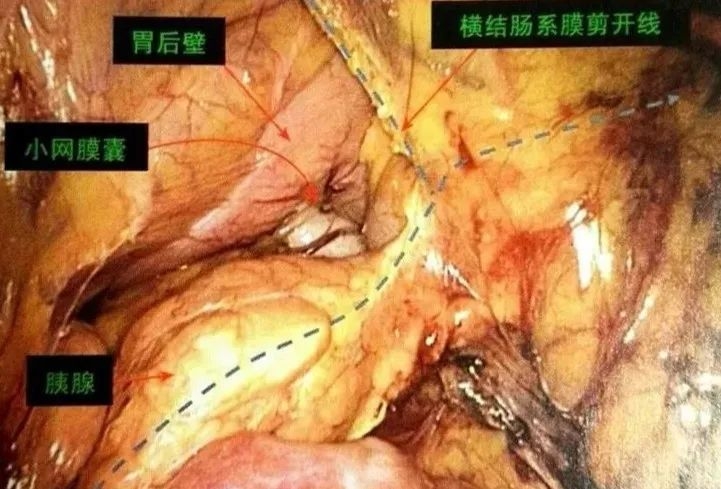
Expose the root of the middle colon blood vessels, clear the lymph nodes, and cut off the left branch
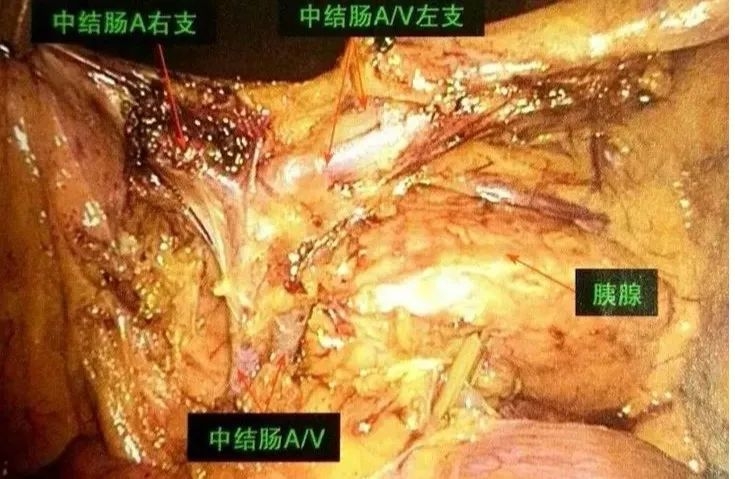
expose the root of the middle colon blood vessels, clear the lymph nodes, and cutoff the left branch

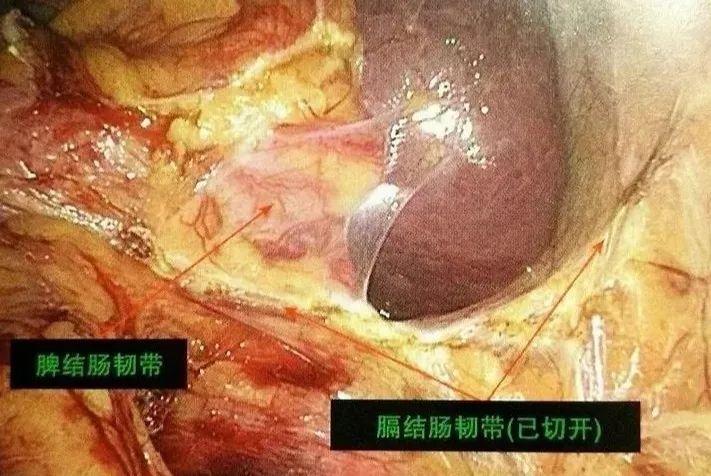
Follow the lateral free splenic flexure
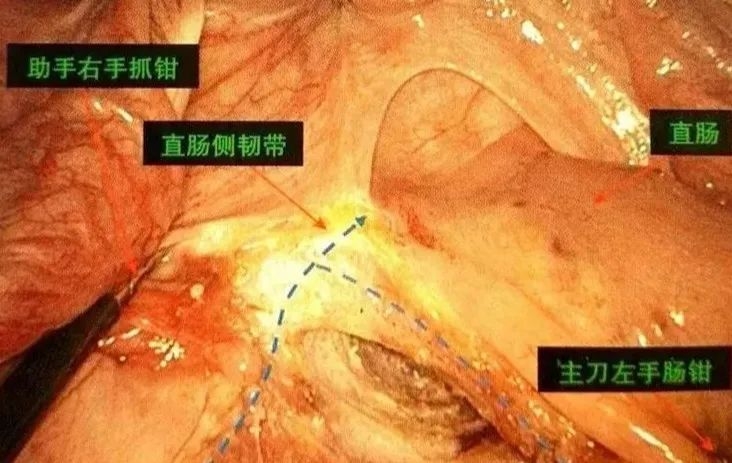
Downward free sigmoid colon, upper rectum
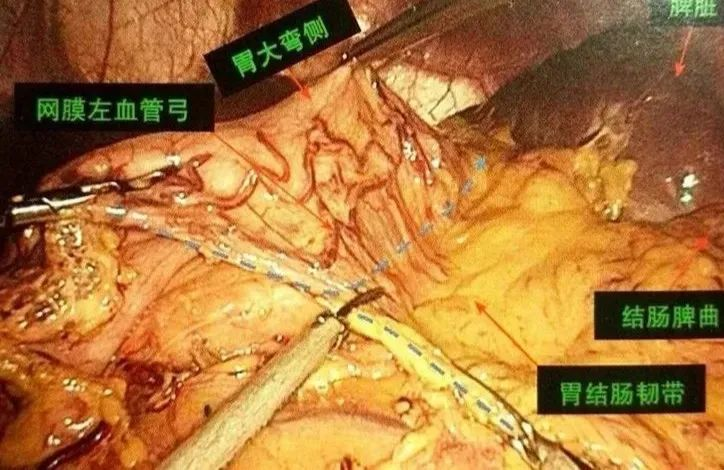
Gastrocolic ligament cut
5.Removal of intestinal segment
After the diseased intestinal segment is completely removed, a small incision about 4-6 cm long is usually made on the belly, and the removed intestine is slowly extracted.
6. Anastomosis of the broken ends and suturing of the incision
The splenic flexure was completely freed, ex vivo resected, and anastomosed.

After the diseased intestinal segment is removed, the incision is sutured and pneumoperitoneum is reestablished. The two intestinal ends are anastomosed under laparoscopy, or the ends are extracted from the incision where the intestine was removed and anastomosed directly, and then put back into the abdominal cavity and the incision is sutured.
In summary, the development of laparoscopic colectomy is a process of continuous progress and innovation. With the continuous maturity of technology and the accumulation of surgeons' experience, it will continue to play an important role in the future.